











7 Cancer Markers in Blood Tests & What You Should Know
Understand the role of cancer markers in blood tests. Learn about common tumour markers in Australia, their limitations, and how they help monitor your health.
Cancer markers can be detected in body fluids such as blood and urine and provide insight into cancer activity. In Australia, blood tests for cancer markers are regularly used in clinical practice to detect known cancers, assess treatment efficacy, determine prognosis, and watch for recurrence. However, their role can be easily misunderstood by patients. How?
While a test for cancer markers is useful, finding these markers during testing does not automatically mean that someone has cancer. Instead, it is one part of a larger diagnostic and treatment-monitoring pathway that also includes clinical assessments, medical imaging, and, often, tissue biopsy.
So, how exactly does detecting cancer markers in a blood test work? What does it mean for your health?
This article will explore how cancer markers work, how they are tested, the common markers tested in Australia, and how doctors use them safely and effectively in real-world medical practice.
Cancer or tumour markers are substances that can be produced by cancers themselves or by normal cells in response to cancer formation. While cancer markers are usually proteins, some can also be hormones, enzymes, or genetic markers associated with cancer activity.
Cancer markers may be found in blood, urine, cancerous tissue, and bone marrow, depending on the type of cancer. Tumour markers are rarely used in isolation to evaluate cancers because they are unreliable on their own. Most of the time, the only way to accurately diagnose cancer is to view the cancerous cells under a microscope. However, tumour markers can confirm that diagnosis, determine the extent of cancer spread, monitor and guide treatment, and detect recurrence. Tumour marker tests are most often used after a cancer diagnosis.
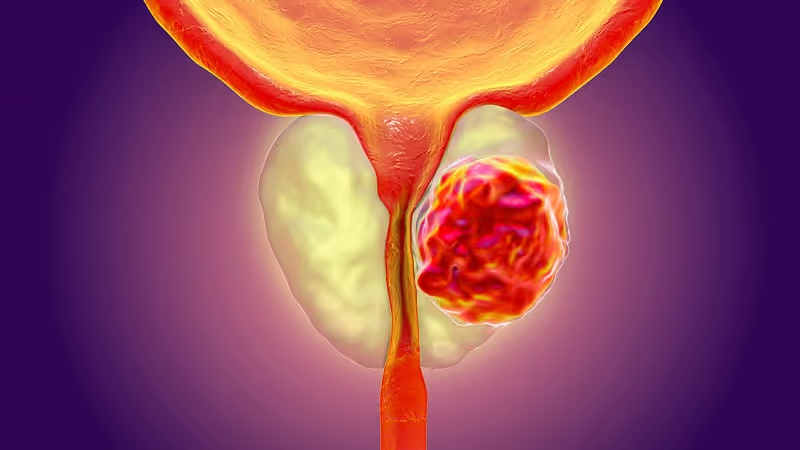
PSA is normally produced by the prostate gland, but its levels rise higher than normal in prostate cancer. Hence, it is used to assess prostate cancer risk, monitor progression and response to treatment, and detect recurrence.
However, a rise in blood PSA levels is not specific to cancer. Levels can rise due to non-cancerous prostate enlargement (benign prostatic hyperplasia), inflammation of the prostate (prostatitis), as well as after medical procedures and recent ejaculation.
Therefore, health professionals may use PSA testing to recommend imaging or a biopsy when indicated. PSA is usually interpreted alongside a person's age, family history, clinical examination and medical imaging. A biopsy usually confirms the diagnosis.
CA-125 is most commonly associated with ovarian cancer and is used to monitor the cancer, assess response to treatment and detect treatment response.
However, it is not used as a screening test because its levels also rise in non-cancerous conditions like endometriosis, liver disease, pregnancy, menstruation and pelvic inflammatory disease.
CEA is often used to assess people with colorectal cancers, but the tumour marker can also be elevated in lung, breast, bladder and pancreatic cancers. It can also be elevated in smokers, inflammatory bowel disease, and other benign gastrointestinal conditions.
Clinicians may commonly use CEA for:
AFP is associated with liver cancers (hepatocellular carcinoma), certain testicular cancers and certain ovarian cancers. Testing for the tumour marker will assist with monitoring tumour progression, treatment assessment and prognosis.
However, AFP levels can also be elevated in hepatitis and chronic liver disease as well as pregnancy.
CA 15-3 levels are most often associated with advanced breast cancers for progression monitoring, treatment response, and recurrence assessment.
However, it is not sensitive enough for early detection and is not used for breast cancer screening.
In small-cell lung cancers, known markers such as neuron-specific enolase (NSE) can be measured to help assess response to treatment; otherwise, other lung cancers rely on imaging and tissue-based genetic markers to guide the selection of targetable therapies.
In blood cancers like multiple myeloma, there will be plasma cell dyscrasia (abnormal protein that can be found in blood or urine), which helps clinicians assess disease burden, response to therapy, and relapse risk.
Cancer marker testing usually involves a simple blood test, such as those used to check general health and organ function. To perform a blood test, a healthcare professional will insert a small needle into a vein to collect a blood sample. This may take only a few minutes and involve very minor discomfort.
Blood samples need to be sent to a specialised laboratory for analysis, and results may take a few days to return.
There is generally no special preparation required. You can eat and drink and take your medicines as usual unless your doctor says otherwise. However, some medications or supplements may affect results (for better or worse), so it is best to inform your healthcare professional in advance.
Cancer markers may also be tested via samples such as:
Remember that testing a sample from the actual suspected cancer is often the only way to confirm cancer, so a biopsy is sometimes needed for the diagnosis of cancer, despite elevated levels of a tumour marker. Sometimes a biopsy is impossible because the tumour's location is inaccessible, or biopsying the tumour can cause severe bleeding or even spread the cancer cells elsewhere. In these situations, a combination of clinical symptoms, diagnostic imaging, and, sometimes, tumour marker testing is sufficient.
One of the most useful applications of tumour markers in Australia is monitoring treatment response.
When levels fall after treatment, it suggests that treatment works. When levels rise, it suggests that the cancer has recurred or progressed and/or that there is increasing resistance to treatment.
Trends over time can often provide more information than a single result. This longitudinal process benefits clinical decision-making by providing prompt alternative strategies to support the best possible patient outcomes.
Not all cancers release markers, and not all people with cancer will have elevated levels of specific markers. Importantly, levels can also be elevated in non-cancerous diseases, inflammatory conditions or after benign processes.
This is why cancer markers are not typically routinely tested for in patients in Australia. Instead, in real-world practice, they are tested for only after diagnosis to best assess treatment options and long-term monitoring.
One of the most important things to understand about cancer marker testing is that it cannot tell you if you have cancer.
There are many reasons for this:
Therefore, imaging tests, a biopsy, associated clinical symptoms and other blood tests (like full blood count or liver function tests) are often used alongside cancer marker tests to assess cancer diagnosis and treatment options.
In many cancers, blood levels of tumour markers at diagnosis or during treatment can suggest prognosis; higher levels or persistent elevations may indicate more aggressive tumours or worse survival (though this is heavily dependent on the individual cancer).
This information benefits clinicians and patients in comparative conversations about treatment goals and expectations.
Tumour marker testing is not a one-size-fits-all approach. Before measuring a tumour marker, clinicians must consider:
Testing without a specific intent can lead to inappropriate measurement, practical implications such as unnecessary worry from false positives/negatives, and flawed interventions due to inappropriate intervention guidance.
Thus, marker tests should only be used when the information gained will provide direct benefit to the patient.
Most cancer marker tests are not appropriate for screening purposes as they may result in false positives, leading to harm from further investigation/biopsy/intervention requests, along with unnecessary psychological distress to patients.
This is why testing is often reserved for monitoring and management, rather than routine screening of asymptomatic patients.
The Everlab program allows you to test for a comprehensive panel of clinically validated biomarkers to identify early disease risk, and incorporates tumour markers when clinically indicated, to deliver a comprehensive picture of your health.
Tumour markers are often touted as a screening test for cancer. While some may be able to detect a disease when used as a sole test, most are not reliable enough for screening. Used in isolation, tumour markers can give false confidence or false warning.
Instead, clinicians consider cancer markers as part of a profile of the patient's overall health, including imaging, complete blood counts, metabolic markers, inflammatory markers, genetic factors for heritable diseases, and personal or familial cancer history.
Cancer marker tests are often ordered alongside other blood tests, including:
These blood tests help assess bone marrow involvement by monitoring changes in blood cells, treatment side effects, and complications such as infection/bleeding.
The Everlab program combines this targeted testing with several other biomarkers, including diagnostic imaging, to give you a holistic picture of your health.
In this way, tumour markers are not used to “screen for cancer”, but rather to inform risk, next steps, and, in some cases, enable earlier decisions based on other objective findings.
Steven is a specialist general practitioner, preventative health consultant, medical educator, healthcare entrepreneur and co-founder of Everlab. With 15+ years of clinical experience, and driven by his passion for preventive care outcomes, Steven is dedicated to personalised and innovative approaches to enhance well-being, extend human lifespan, and improve healthspan.



Join 1000's of Australians improving their health with proactive, personalised healthcare.
